 Overview OverviewEssentially, there's one consistent type of Hammer toe, the condition in which your toes are contracted into a hammer or upside-down "V" shape. However, depending on its severity, hammertoe is characterized into two forms. Flexible hammertoe is hammertoe in which the joints of the toes are still moveable or flexible and can be treated with nonsurgical therapies. Rigid hammertoe is the more serious condition in which the joints' muscles and tendons have lost any flexibility and the contraction cannot be corrected by nonsurgical means. As a result, surgery is generally required to deal with the problem. This is why it's important to consult a physician as soon as the problem is recognized for the possibility of successful nonsurgical treatment. Causes People who are born with long bones in their toes are more likely to develop hammer toe. Children who wear shoes they have outgrown may develop this condition. People who wear very narrow shoes or high-heeled shoes are also more likely to develop a hammer toe. Sometimes, pressure from a bunion can cause hammer toe. Rheumatoid arthritis is another a risk factor.  Symptoms SymptomsThe symptoms of a hammer toe are usually first noticed when a corn develops on the top of the toe and becomes painful, usually when wearing tight shoes. There may be a bursa under the corn or instead of a corn, depending on the pressure. Most of the symptoms are due to pressure from footwear on the toe. There may be a callus under the metatarsal head at the base of the toe. Initially a hammer toe is usually flexible, but when longstanding it becomes more rigid. Diagnosis Hammertoes are progressive, they don?t go away by themselves and usually they will get worse over time. However, not all cases are alike, some hammertoes progress more rapidly than others. Once your foot and ankle surgeon has evaluated your hammertoes, a treatment plan can be developed that is suited to your needs. Non Surgical Treatment If the problem is caught in the early stages you can avoid hammer toe surgery. One of the easiest methods of treatment is to manipulate the toe out of a bent position then splint and buddy wrap it alongside it?s larger neighbour. This method of hammer toe taping will help the problem to fix itself. Make sure the toe isn?t resuming its bent shape during the recovery. To alleviate some of the painful symptoms of hammer toe avoid wearing high heels or shoes that cramp or stifle your feet. Choosing a pair of minimalist shoes can be an excellent choice for both foot and postural health. Wearing shoes that give the toes plenty of space and are comfortable lined is also a smart choice. Hammer toe recovery starts be treating the toe respectfully. Soft insoles or protection for the corn can also provide additional assistance. Surgical Treatment Hammertoe surgery is performed when conservative measures have been exhausted and pain or deformity still persists. The surgery is performed on an outpatient basis. It typically required about one hour of time. An incision is placed over the inter-phalangeal joint. Once the bone is exposed, the end portion of the bone is removed. Your surgeon may then use pins or other fixation devices to assist in straightening the toe. These devices may be removed at a later date if necessary. Recovery for hammertoe surgery is approximately 10 to 14 days. You are able to walk immediately following the surgery in a surgical shoe. Swelling may be present but is managed as needed. Physical therapy is used to help reduce swelling in the toe or toes after surgery. Most of these toe surgeries can hammertoe be performed in the office or the outpatient surgery under local anesthesia.  Prevention PreventionThe number-one hammertoe prevention tip is to wear properly fitting shoes. If your shoes feel too snug, go to your local shoe store and have the length and width of your feet measured. If you wear high heels, keep the heel height to 2 inches or less. Wearing shoes with high heels increases the pressure on your toes and causes them to bend. It can also cause the formation of corns and a high arch. Overview
Pronation is a turning outward of the foot at the ankle, which allows the foot to flatten. The pronation helps to absorb some of the compressive shock forces, torque conversion, adjustment to uneven ground contours, and maintenance of balance. It is necessary to have a certain amount of pronation to disseminate the energy of the foot-strike. If there is too little or too much pronation injuries may occur. When a foot and ankle pronates to a great degree, we call it over-pronation. Normally you can see the Achilles Tendon run straight down the leg into the heel. If the foot is over-pronated, the tendon will run straight down the leg, but when it lies on the heel it will twist outward. This makes the inner ankle bone much more prominent than the outer ankle bone.  Causes Congenital "Flat Feet" - an individual may be born with feet that lack an appropriately supportive arch thereby predisposing the individual to this foot condition. Excessive Weight (Obesity) Too much weight on the foot from either obesity or pregnancy may be a factor. Repetitive Impact walking on flat, hard surfaces continuously places unnatural stress on the foot arch. Symptoms When standing, your heels lean inward. When standing, one or both of your knee caps turn inward. Conditions such as a flat feet or bunions may occur. You develop knee pain when you are active or involved in athletics. The knee pain slowly goes away when you rest. You abnormally wear out the soles and heels of your shoes very quickly. Diagnosis If you have flat feet or low arches, chances are you overpronate. Although not always the case, the lower your arches the greater the overpronate. Stand on a hard surface (in front of a mirror if you need to) and look at your feet, flat feet or low arches are easy to spot. If your feet look flatter than a pancake, have a look at your ankles and see if they seem collapsed or straight. If they are, you're overpronating.  Non Surgical Treatment Anti-Pronation Insoles provide a unique foot support system that aligns the lower body. The major cause of foot and leg pain is over pronation (rolling over of the feet) which causes excessive pressure on the muscles, ligaments and bones of the lower body. Running insoles treat the underlying cause of over pronation and prevent future occurrences of the associated foot or leg condition. A project conducted at the NIKE Sport Research Laboratory studied the effects of orthotics on rear foot movement in running. Nine well-trained runners who wore orthotics were chosen as subjects. The results of the study indicated that orthotics reduced rear foot movement by roughly one degree or approximately nine percent of the amount found in runners not using orthotics. The average reduction of the maximum velocity of pronation was fifteen percent. Thus this study indicates that orthotics and insoles control over pronation which will treat and prevent many sporting injuries. Surgical Treatment Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. Overview
Sever?s disease, also referred to as calcaneal apophysitis, is an injury in the growth plate of the lower part of the heel bone where the Achilles tendon attaches to the bone. Sever?s disease is a common condition affecting children between the ages of 8 and 15 that participate in sports or are particularly active. This condition is believed to be caused by repeated trauma to the heel, weakening its internal structure. Typically occurring in adolescence, Sever?s disease causes painful inflammation of the growth plate. This condition can affect any child, however there is a higher probability of its occurrence if the child experiences pronation, has flat or high arches, short leg syndrome and/or is overweight. Causes Overuse and stress on the heel bone through participation in sports is a major cause of calcaneal apophysitis. The heel?s growth plate is sensitive to repeated running and pounding on hard surfaces, resulting in muscle strain and inflamed tissue. For this reason, children and adolescents involved in soccer, track, or basketball are especially vulnerable. Other potential causes of calcaneal apophysitis include obesity, a tight Achilles tendon, and biomechanical problems such as flatfoot or a high-arched foot. Symptoms Symptoms include complaints of pain or tenderness in the heel (or heels), discomfort when heel is squeezed, limping, and more severe pain after walking, running or playing sports. Sever?s disease is directly related to overuse of the bone and tendons in the heel. This can come from playing sports or anything that involves lots of heel movements and hard shoes such as cleats. It can be associated with starting a new sport, or the start of a new season. It occurs more commonly in children who pronate (feet roll inward), and involves both heels in more than half of patients. Diagnosis Sever?s disease can be diagnosed based on your history and symptoms. Clinically, your physiotherapist will perform a "squeeze test" and some other tests to confirm the diagnosis. Some children suffer Sever?s disease even though they do less exercise than other. This indicates that it is not just training volume that is at play. Foot and leg biomechanics are a predisposing factor. The main factors thought to predispose a child to Sever?s disease include decrease ankle dorsiflexion, abnormal hind foot motion eg overpronation or supination, tight calf muscles, excessive weight-bearing activities eg running. Non Surgical Treatment Sever?s disease will go away on its own with rest or after heel bone growth is complete, usually within 2 to 8 weeks after the heel pain or discomfort appears. Sever?s disease is not expected to cause long-term problems, though symptoms may linger for up to several years in severe cases. Certain conservative care measures may be helpful in treating this health problem, including avoiding activities that provoke pain or discomfort, elevating the leg while at rest, performing hamstring and calf muscle stretches two to three times per day, undergoing physical therapy, using cold therapy, using an elastic wrap or compression stocking, Avoiding footwear with heel elevation, toe spring, and toe taper, and instead favoring footwear that?s completely flat and widest at the ends of the toes. More aggressive treatment measures, including over-the-counter anti-inflammatory medication (e.g. ibuprofen), steroid injections, and surgery, may be indicated in certain cases. Addressing the footwear component of this health problem is an important part of a well-rounded Sever?s disease treatment plan. Optimal footwear for preventing or treating this problem is flat, wide (widest at the ends of the toes), and flexible in the sole. Open-back footwear (such as certain Crocs models) may be particularly helpful for kids and teens with Sever?s disease. Surgical Treatment The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Overview
 Achilles Tendon Rupture Surgery is a surgical procedure is used to repair a ruptured Achilles tendon. There are two types of surgery an open surgery and a percutaneous surgery, in both cases the surgeon sews the tendon back together through the incision helping the tendon to heal properly and restore function to the foot and ankle. If the injury or rupture has caused severe swelling the surgery may be delayed for a short period of time to allow the swelling to go down. Achilles Tendon Rupture Surgery is a surgical procedure is used to repair a ruptured Achilles tendon. There are two types of surgery an open surgery and a percutaneous surgery, in both cases the surgeon sews the tendon back together through the incision helping the tendon to heal properly and restore function to the foot and ankle. If the injury or rupture has caused severe swelling the surgery may be delayed for a short period of time to allow the swelling to go down.Causes The cause of Achilles tendon ruptures besides obviously direct trauma, is multifactorial. In many instances the rupture occurs about 2-6 cm before its attachment to the calcaneous (heel bone). In this area there is a weaker blood supply making it more susceptible to injury and rupture. Rigid soled shoes can also be the causative factor in combination with the structure of your foot being susceptible to injury. Symptoms Symptoms of an Achilles tendon injury are as follows. Pain along the back of your foot and above your heel, especially when stretching your ankle or standing on your toes; with tendinitis, pain may be mild and worsen gradually. If you rupture the tendon, pain can be abrupt and severe. Tenderness. Swelling. Stiffness. Hearing a snapping or popping noise during the injury. Difficulty flexing your foot or pointing your toes (in complete tears of the tendon). Diagnosis It is usually possible to detect a complete rupture of the Achilles tendon on the history and examination. A gap may be felt in the tendon, usually 4-5cm above the heel bone. This is the normal site of injury and is called an intra-substance tear. The tear can occur higher up about 10cm above the insertion into the heel at the site where the muscles join the tendon, this is known as a musculo-tendinous tear. A special test will be performed which involves squeezing the calf. Normally if the Achilles tendon is intact this causes the foot to point downwards but if it is ruptured it causes no movement. To confirm the diagnosis and the exact site of the rupture it may be necessary to perform an Ultra-sound or MRI scan. Non Surgical Treatment The other option is to allow your tendon to heal without surgery. In this case, you also need to wear a cast, splint, walking boot, or brace for 6-8 weeks. You also may have different exercises to do. If you are less active or have a chronic illness that prevents surgery, this option may be better for you.  Surgical Treatment Regaining Achilles tendon function after an injury is critical for walking. The goal of Achilles tendon repair is to reconnect the calf muscles with the heel bone to restore push-off strength. Those best suited for surgical repair of an acute or chronic Achilles tendon rupture include healthy, active people who want to return to activities such as jogging, running, biking, etc. Even those who are less active may be candidates for surgical repair. Non-operative treatment may also be an option. The decision to operate should be discussed with your orthopaedic foot and ankle surgeon. Overview
Bone growth restriction (epiphysiodesis) The objective of this surgical procedure is to slow down growth in the longer leg. During surgery, doctors alter the growth plate of the bone in the longer leg by inserting a small plate or staples. This slows down growth, allowing the shorter leg to catch up over time. Your child may spend a night in the hospital after this procedure or go home the same day. Doctors may place a knee brace on the leg for a few days. It typically takes 2 to 3 months for the leg to heal completely. An alternative approach involves lengthening the shorter bone. We are more likely to recommend this approach if your child is on the short side of the height spectrum.  Causes The causes of LLD may be divided into those that shorten a limb versus those that lengthen a limb, or they may be classified as affecting the length versus the rate of growth in a limb. For example, a fracture that heals poorly may shorten a leg slightly, but does not affect its growth rate. Radiation, on the other hand, can affect a leg's long-term ability to expand, but does not acutely affect its length. Causes that shorten the leg are more common than those that lengthen it and include congenital growth deficiencies (seen in hemiatrophy and skeletal dysplasias ), infections that infiltrate the epiphysis (e.g. osteomyelitis ), tumors, fractures that occur through the growth plate or have overriding ends, Legg-Calve-Perthes disease, slipped capital femoral epiphysis (SCFE), and radiation. Lengthening can result from unique conditions, such as hemihypertrophy , in which one or more structures on one side of the body become larger than the other side, vascular malformations or tumors (such as hemangioma ), which cause blood flow on one side to exceed that of the other, Wilm's tumor (of the kidney), septic arthritis, healed fractures, or orthopaedic surgery. Leg length discrepancy may arise from a problem in almost any portion of the femur or tibia. For example, fractures can occur at virtually all levels of the two bones. Fractures or other problems of the fibula do not lead to LLD, as long as the more central, weight-bearing tibia is unaffected. Because many cases of LLD are due to decreased rate of growth, the femoral or tibial epiphyses are commonly affected regions. Symptoms The effects vary from patient to patient, depending on the cause of the discrepancy and the magnitude of the difference. Differences of 3 1/2 to 4 percent of the total length of the lower extremity (4 cm or 1 2/3 inches in an average adult), including the thigh, lower leg and foot, may cause noticeable abnormalities while walking and require more effort to walk. Differences between the lengths of the upper extremities cause few problems unless the difference is so great that it becomes difficult to hold objects or perform chores with both hands. You and your physician can decide what is right for you after discussing the causes, treatment options and risks and benefits of limb lengthening, including no treatment at all. Although an LLD may be detected on a screening examination for curvature of the spine (scoliosis), LLD does not cause scoliosis. There is controversy about the effect of LLD on the spine. Some studies indicate that people with an LLD have a greater incidence of low back pain and an increased susceptibility to injuries, but other studies refute this relationship. Diagnosis The only way to decipher between anatomical and functional leg length inequalities (you can have both) is by a physical measurement and series of biomechanical tests. It is actually a simple process and gets to the true cause of some runner?s chronic foot, knee, hip and back pain. After the muscles are tested and the legs are measured it may be necessary to get a special X-ray that measures both of your thighs (Femurs) and legs (Tibias). The X-ray is read by a medical radiologist who provides a report of the actual difference down to the micrometer leaving zero room for error. Once the difference in leg length is known, the solution becomes clear. Non Surgical Treatment The non-surgical intervention is mainly usedfor the functional and environmental types of leg length discrepancies. It is also applied to the mild category of limb length inequality. Non-surgical intervention consists of stretching the muscles of the lower extremity. This is individually different, whereby the M. Tensor Fascia latae, the adductors, the hamstring muscles, M. piriformis and M. Iliopsoas are stretched. In this non-surgical intervention belongs also the use of shoe lifts. These shoe lifts consists of either a shoe insert (up to 10-20mm of correction), or building up the sole of the shoe on the shorter leg (up to 30-60mm of correction). This lift therapy should be implemented gradually in small increments. Several studies have examined the treatment of low back pain patients with LLD with shoe lifts. Gofton obtained good results: the patients experienced major or complete pain relief that lasted upon follow-up ranging from 3 to 11 years. Helliwell also observed patients whereby 44% experienced complete pain relief, and 45% had moderate or substantial pain relief. Friberg found that 157 (of 211) patients with LBP, treated with shoe lifts, were symprom-free after a mean follow-up of 18 months.  Surgical Treatment Surgeries for LLD are designed to do one of three general things ? shorten the long leg, stop or slow the growth of the longer or more rapidly growing leg, or lengthen the short leg. Stopping the growth of the longer leg is the most commonly utilized of the three approaches and involves an operation known as an epiphysiodesis , in which the growth plate of either the lower femur or upper tibia is visualized in the operating room using fluoroscopy (a type of real-time radiographic imaging) and ablated , which involves drilling into the region several times, such that the tissue is no longer capable of bone growth. Because the epiphyseal growth capabilities cannot be restored following the surgery, proper timing is crucial. Usually the operation is planned for the last 2 to 3 years of growth and has excellent results, with children leaving the hospital within a few days with good mobility. However, it is only appropriate for LLD of under 5cm.
Overview
Adult-acquired flatfoot is a challenging condition to treat. It is defined as a symptomatic, progressive deformity of the foot caused by loss of supportive structures of the medial arch. It is becoming increasingly frequent with the aging population and the obesity epidemic. Patients commonly try to lose weight by exercising to improve the condition. This often leads to worsening of symptoms and progression of the disorder. Early recognition of this complex disorder is essential, if chronic pain and surgery are to be avoided.  Causes Flat feet causes greater pressure on the posterior tibial tendon than normal. As the person with flat feet ages, the muscles, tendons and ligaments weaken. Blood supplies diminish as arteries narrow. These conditions are magnified for obese patients because of their increased weight and atherosclerosis. Finally, the tendon gives out or tears. Most of the time, this is a slow process. Once the posterior tibial tendon and ligaments stretch, body weight causes the bones of the arch to move out of position. The foot rotates inward (pronation), the heel bone is tilted to the inside, and the arch appears collapsed. In some cases, the deformity progresses until the foot dislocates outward from the ankle joint. Symptoms The symptoms of PTTD may include pain, swelling, a flattening of the arch, and inward rolling of the ankle. As the condition progresses, the symptoms will change. For example, later, as the arch begins to flatten, there may still be pain on the inside of the foot and ankle. But at this point, the foot and toes begin to turn outward and the ankle rolls inward. As PTTD becomes more advanced, the arch flattens even more and the pain often shifts to the outside of the foot, below the ankle. The tendon has deteriorated considerably and arthritis often develops in the foot. In more severe cases, arthritis may also develop in the ankle. Symptoms, which may occur in some persons with flexible flatfoot, include. Pain in the heel, arch, ankle, or along the outside of the foot. ?Turned-in? ankle. Pain associated with a shin splint. General weakness / fatigue in the foot or leg. Diagnosis Observe forefoot to hindfoot alignment. Do this with the patient sitting and the heel in neutral, and also with the patient standing. I like to put blocks under the forefoot with the heel in neutral to see how much forefoot correction is necessary to help hold the hindfoot position. One last note is to check all joints for stiffness. In cases of prolonged PTTD or coalition, rigid deformity is present and one must carefully check the joints of the midfoot and hindfoot for stiffness and arthritis in the surgical pre-planning. Non surgical Treatment PTTD is a progressive condition. Early treatment is needed to prevent relentless progression to a more advanced disease which can lead to more problems for that affected foot. In general, the treatments include rest. Reducing or even stopping activities that worsen the pain is the initial step. Switching to low-impact exercise such as cycling, elliptical trainers, or swimming is helpful. These activities do not put a large impact load on the foot. Ice. Apply cold packs on the most painful area of the posterior tibial tendon frequently to keep down the swelling. Placing ice over the tendon immediately after completing an exercise helps to decrease the inflammation around the tendon. Nonsteroidal Anti-inflammatory Medication (NSAIDS). Drugs, such as arcoxia, voltaren and celebrex help to reduce pain and inflammation. Taking such medications prior to an exercise activity helps to limit inflammation around the tendon. However, long term use of these drugs can be harmful to you with side effects including peptic ulcer disease and renal impairment or failure. Casting. A short leg cast or walking boot may be used for 6 to 8 weeks in the acutely painful foot. This allows the tendon to rest and the swelling to go down. However, a cast causes the other muscles of the leg to atrophy (decrease in strength) and thus is only used if no other conservative treatment works. Most people can be helped with orthotics and braces. An orthotic is a shoe insert. It is the most common non-surgical treatment for a flatfoot and it is very safe to use. A custom orthotic is required in patients who have moderate to severe changes in the shape of the foot. Physiotherapy helps to strengthen the injured tendon and it can help patients with mild to moderate disease of the posterior tibial tendon.  Surgical Treatment Surgical correction is dependent on the severity of symptoms and the stage of deformity. The goals of surgery are to create a more functional and stable foot. There are multiple procedures available to the surgeon and it may take several to correct a flatfoot deformity. Usually surgical treatment begins with removal of inflammatory tissue and repair of the posterior tibial tendon. A tendon transfer is performed if the posterior tibial muscle is weak or the tendon is badly damaged. The most commonly used tendon is the flexor digitorum longus tendon. This tendon flexes or moves the lesser toes downward. The flexor digitorum longus tendon is utilized due to its close proximity to the posterior tibial tendon and because there are minimal side effects with its loss. The remainder of the tendon is sutured to the flexor hallucis longus tendon that flexes the big toe so that little function is loss.
Overview
The posterior tibial tendon serves as one of the major supporting structures of the foot, helping it to function while walking. Posterior tibial tendon dysfunction (PTTD) is a condition caused by changes in the tendon, impairing its ability to support the arch. This results in flattening of the foot. PTTD is often called ?adult acquired flatfoot? because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. PTTD is usually progressive, which means it will keep getting worse, especially if it isn?t treated early.  Causes Flat feet causes greater pressure on the posterior tibial tendon than normal. As the person with flat feet ages, the muscles, tendons and ligaments weaken. Blood supplies diminish as arteries narrow. These conditions are magnified for obese patients because of their increased weight and atherosclerosis. Finally, the tendon gives out or tears. Most of the time, this is a slow process. Once the posterior tibial tendon and ligaments stretch, body weight causes the bones of the arch to move out of position. The foot rotates inward (pronation), the heel bone is tilted to the inside, and the arch appears collapsed. In some cases, the deformity progresses until the foot dislocates outward from the ankle joint. Symptoms Many patients with this condition have no pain or symptoms. When problems do arise, the good news is that acquired flatfoot treatment is often very effective. Initially, it will be important to rest and avoid activities that worsen the pain. Diagnosis Diagnostic testing is often used to diagnose the condition and help determine the stage of the disease. The most common test done in the office setting are weightbearing X-rays of the foot and ankle. These assess joint alignment and osteoarthritis. If tendon tearing or rupture is suspected, the gold standard test would be MRI. The MRI is used to check the tendon, surrounding ligament structures and the midfoot and hindfoot joints. An MRI is essential if surgery is being considered. Non surgical Treatment Depending on the stage of the deformity and patient?s functional goals, various treatment options are available. Some patients improve with conservative care which includes rest and immobilization, shoe modifications, orthoses and bracing, or physical therapy. Surgery might be warranted for advanced stages of the condition. Often a combination of procedures including tendon and muscle augmentation, tendon transfers, realigning of bones or fusion of certain joints might be necessary in more advanced cases. Your doctor will evaluate and recommend an individualized plan of care with your specific needs in mind. 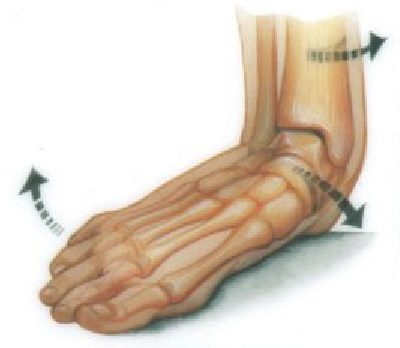 Surgical Treatment For those patients with PTTD that have severe deformity or have not improved with conservative treatments, surgery may be necessary to return them to daily activity. Surgery for PTTD may include repair of the diseased tendon and possible tendon transfer to a nearby healthy tendon, surgery on the surrounding bones or joints to prevent biomechanical abnormalities that may be a contributing factor or both. |
